The Chronic Pain Conundrum–Conclusion
Continued from yesterday.
Early refill requests from patients, short tempers, and demands for their medicine in spite of legal restrictions, are red flags pointing to addiction and non-therapeutic requirements for dangerous substances. Dealing with people who behave like this frequently cause pharmacy staffs to become jaundiced and suspicious of customers who take a lot of pain medication. It’s an unfortunate situation and has gotten worse in the last two decades.
 Flash back twenty years to the late nineties. A doctor friend of mine back in Louisiana was getting a less than favorable reputation with the local pharmacists. Several were refusing to fill his prescriptions. I invited him to breakfast one day and my main point was, “If you aren’t careful with your prescribing habits, your reputation will continue to deteriorate, and what’s worse, a fleet of black Suburbans will arrive at your front door and they won’t be there to help.” Needless to say, the mood of our breakfast meeting turned somber in the wink of an eye. He said, “That’s already happened. Let me assure you, I’m doing my homework. Almost ninety per cent of my patients are referrals from other doctors. These patients arrive with extensive charts, detailed notes, and X-rays. I’m covering my ass.” I said, “Then you should do some PR with the local pharmacists or your patients are going to have a hard time getting their prescriptions filled.”
Flash back twenty years to the late nineties. A doctor friend of mine back in Louisiana was getting a less than favorable reputation with the local pharmacists. Several were refusing to fill his prescriptions. I invited him to breakfast one day and my main point was, “If you aren’t careful with your prescribing habits, your reputation will continue to deteriorate, and what’s worse, a fleet of black Suburbans will arrive at your front door and they won’t be there to help.” Needless to say, the mood of our breakfast meeting turned somber in the wink of an eye. He said, “That’s already happened. Let me assure you, I’m doing my homework. Almost ninety per cent of my patients are referrals from other doctors. These patients arrive with extensive charts, detailed notes, and X-rays. I’m covering my ass.” I said, “Then you should do some PR with the local pharmacists or your patients are going to have a hard time getting their prescriptions filled.”
Flash back to 1979, again in Louisiana.
A team of undercover agents arrives at a doctor’s office and is greeted by the front desk person seated in the apex of a V-shaped desk. On either side of the desk, leading in separate directions were two doors. After a friendly greeting, she asked, “Are you on a diet, or are you in pain?” Not a good beginning. That prescriber eventually lost the privilege of writing prescriptions.
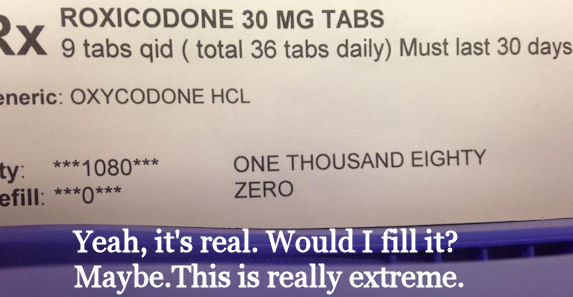
There’s nothing new under the sun—and because of the abuse potential, pharmacists are now apt to scrutinize every pain prescription more closely, whether it’s a C-2,3, or 4 drug.
I haven’t heard from Alpha again, although it is safe to predict that she found a pharmacist to fill her prescriptions.
Never heard from Mr. Epsilon again either. If he isn’t in jail, I hope he’s in some kind of recovery program.
Gamma’s saving grace is that all of her meds are being prescribed by the same doctor, an oncologist.

Many pain clinics are simply store fronts for unscrupulous doctors engaged in diversion.
Beta is another story. Beta now lives in Tennessee, sees a doctor in a strip mall in Florida, and uses pharmacies in Georgia and Kentucky. He’s not on the peace train, he’s riding the Oxycontin Express.
When there’s so many bad apples, perhaps it’s time to examine the orchard.
Acknowledgement: Free lance writer and investigative reporter, George McGinn contributed to this article.
Future blog topics: “What is the ‘Oxycontin Express'” and “Why won’t you fill my prescription?”
 March 22, 2015
March 22, 2015 FCEtier
FCEtier